《Slide 4.》Brain abscess, Cerebrum
A. Brief Descriptions:
-
Types:
-
Emboli cerebral abscess from infected foci in body 40%.
-
Direct extension of cerebral abscess from adjacent infected foci.
-
Relate to cerebral trauma, 30%.
-
Idiopathic abscess, 20%.
-
-
Stages :
Infected thromboembolus forming a necrotic foci.
Acute cerebritis.
Liquefaction & purulent exudates.
Heavy infiltration (2 days).
Granulation at margins (5-7 days).
Encapsulation.
B. Gross Findings:
-
Discrete lesions with central liquefactive necrosis, surrounding by fibrous, collagenized response and edema.
C. Micro Findings:
-
Necrotic, purulent center.
-
Capsule of granulomatous tissue & fibrosis (capillaries proliferation, infiltration, Gitter cells...).
-
Surrounding reactive brain with edema & gliosis.
D. Others:
-
Cerebritis: focal inflammation of brain parenchyma.
-
Myelitis: focal inflammation of spinal cord.
-
Focal pyogenic cerebritis.
-
Emboli suppurative encephalitis.
E. Reference:
-
Robbins Pathologic Basis of Disease, 6th ed. P.349-352.
|
|
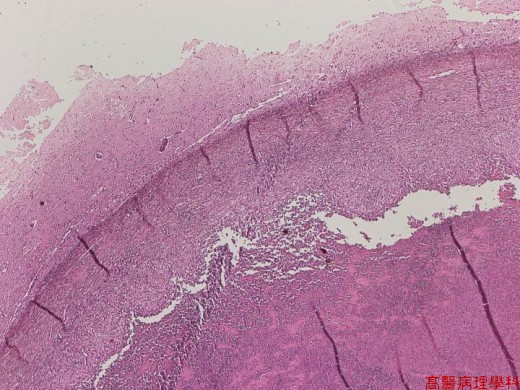
【 Fig. 4-1 (LP)】The normal architecture of cerebrum is destructed.
|
|

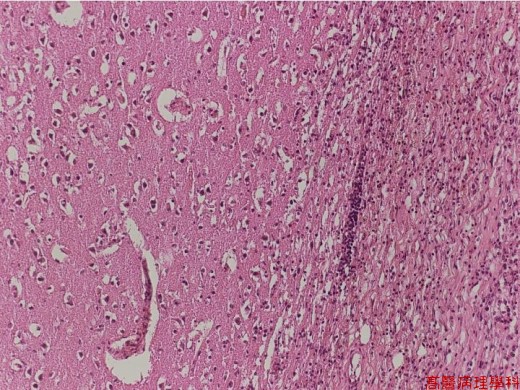
【 Fig. 4-2 (LP)】The necrotic area is in the left, the normal cerebral cortex in the right, and a thick fibrous band lined between them.
|
|
【 Fig. 4-3 (LP)】The normal cerebral cortex (left) and the fibrous capsule (right) surrounding the necrotic area (not shown here). Note the rather dense and parallel fibrous bundles of the capsule.
|
|
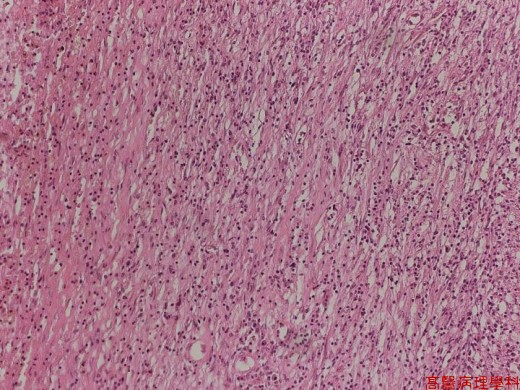
【 Fig. 4-4 (LP)】The fibrous capsule. Note the more outside of the capsule (left side in this picture), the more thickening of the fibrous bundles.
|
|
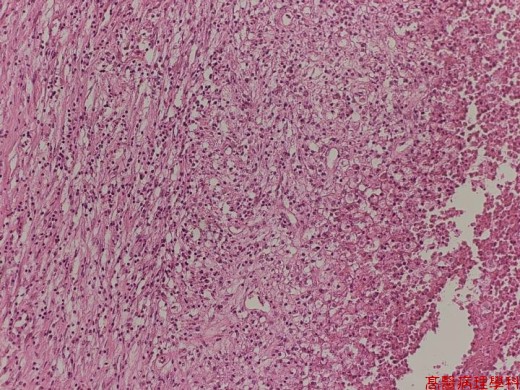
【 Fig. 4-5 (LP)】The necrotic center (right) is surrounded by granulation tissue (left). Note foamy histiocytes (Gitter cells) aggregate in the outermost of the necrotic area.
|
|
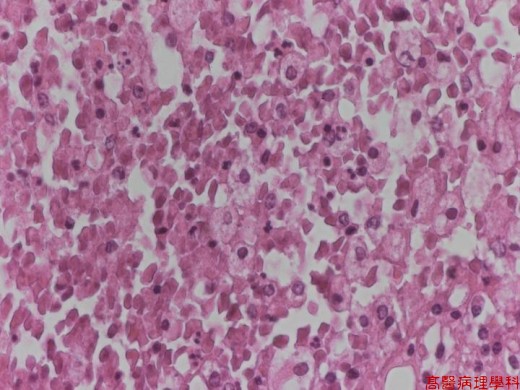
【 Fig. 4-6 (HP)】The necrotic area is composed of cell debris, nuclear dusts, inflammatory cells (most frequently PMNs) and Gitter cells (foamy histiocytes in the CNS).
![]()
![]()
![]()